J. Biosci. Public Health. 2026; 2(2)
First Author
![]() https://orcid.org/0000-0003-4832-2626
https://orcid.org/0000-0003-4832-2626
Affiliations:
Department of Nutrition and Food Engineering, Daffodil International University, Birulia-1216,Bangladesh
Coauthor
![]() ORCID: https://orcid.org/0000-0002-7686-7749
ORCID: https://orcid.org/0000-0002-7686-7749
Affiliations:
Department of Mathematical and Physical Sciences, East West University, Dhaka-1212, Bangladesh
Coauthor
![]() ORCID: https://orcid.org/0000-0003-4903-3690
ORCID: https://orcid.org/0000-0003-4903-3690
Affiliations:
Department of Public Health, Daffodil International University, Birulia-1216, Bangladesh
Coauthor
![]() ORCID: https://orcid.org/0009-0003-0559-8523
ORCID: https://orcid.org/0009-0003-0559-8523
Affiliations:
Department of Public Health, University of Science and Technology Chittagong, Chattogram-4202, Bangladesh
Corresponding Author *
![]() https://orcid.org/0000-0003-4903-3690
https://orcid.org/0000-0003-4903-3690
Affiliations:
Department of Public Health, University of Science and Technology Chittagong, Chattogram-4202, Bangladesh
Corresponding Author *
![]() https://orcid.org/0000-0003-4903-3690
https://orcid.org/0000-0003-4903-3690
Affiliations:
Department of Public Health, University of Science and Technology Chittagong, Chattogram-4202, Bangladesh
Diarrheal disease remains a leading cause of morbidity among children under five years in low- and middle-income countries, including Bangladesh. Water, sanitation, and hygiene (WASH) practices are key determinants influencing disease transmission. This study aimed to assess the prevalence of diarrheal disease among under-five children in Chattogram, Bangladesh, and its association with maternal and household WASH practices. A cross-sectional study was conducted among 182 mothers attending two hospitals in Chattogram city through a random sampling method. A high recent prevalence of diarrhea was reported, with 69.2% of children experiencing an episode within the last five months. Only 37.4% of households had ideal sanitary facilities. Significant associations were found between diarrheal frequency and sanitation factors with significance set at p<0.05: toilet cleanliness (p<0.007), toilet type (p<0.003), cleaning frequency (p<0.002), and sewage channel availability (p<0.01). Hygiene practices were also significantly associated, including handwashing after defecation (p<0.002), washing produce before consumption/cooking (p<0.000), handwashing before/after eating (p<0.02), and the type of soap used (p<0.02). A notable 41.8% of households used no water purification method. 71.4% of mothers reported using antibiotics alongside oral rehydration therapy. Regression analysis revealed that more frequent toilet cleaning (p=0.070, 95% CI: -0.600 to 0.024) and regular handwashing (p=0.069, 95% CI: -1.848 to 0.071) were associated with fewer diarrheal episodes. WASH-related maternal hygiene behaviors and household sanitation conditions are significant determinants of diarrheal disease among under-five children in urban Bangladesh. Interventions focusing on sustained behavior change, improved sanitation practices, and rational antibiotic use are essential to reduce disease burden.
Diarrheal disease remains a major cause of preventable morbidity and mortality among children younger than five years globally. Defined as the passage of three or more loose or liquid stools per day [1], diarrhea accounts for approximately 7·3% of all under-five deaths and ranks as the third leading cause of mortality worldwide, and the second in the WHO South-East Asia Region [1, 2]. Each year, an estimated 1·7 billion episodes of diarrhea occur among children, resulting in approximately 443,800 deaths [1, 3]. The burden is disproportionately high in low- and middle-income countries, where factors such as poor sanitation and lack of access to safe drinking water are major contributors [4–6]. Indeed, unsafe water and poor sanitation are implicated in 72% and 56% of diarrheal deaths, respectively, with improvements in Water, Sanitation, and Hygiene (WASH) practices having the potential to avert a significant portion of the global disease burden [7]. Robust evidence underscores the critical role of WASH in diarrheal prevention. Handwashing with soap at critical times such as after toilet use, after handling child excreta, and before food preparation and feeding is one of the most effective interventions [8–11]. Enhanced access to safe water, improved sanitation facilities, and proper hygiene behaviors can interrupt the fecal-oral transmission pathway, reducing diarrhea risk substantially [6, 7]. Studies consistently link poor WASH practices, including inadequate handwashing and unsafe water handling, to a higher prevalence of childhood diarrhea [12–15]. Conversely, interventions like community-led total sanitation and hygiene (CLTSH) have been associated with reduced diarrhea risk [16].
In Bangladesh, diarrheal disease is a persistent public health challenge. A prior study indicated that 46% of children experienced at least one diarrheal episode within a two-week period [17], with children aged 12-23 months in rural areas being particularly vulnerable [18]. While national efforts have improved WASH indicators, disparities in access and consistent practice persist [19, 20]. Chattogram, one of the largest and rapidly urbanizing cities in Bangladesh, presents a unique context where population density, informal settlements, and infrastructural constraints may exacerbate WASH-related risks. Rapid urbanization often places significant pressure on water supply systems, sanitation infrastructure, and waste management services, potentially increasing the risk of diarrheal diseases among young children. However, there is a research gap in localized, contemporary evidence specifically examining the association between maternal WASH practices and diarrheal infection among under-five children within this urban context. Previous studies in similar settings have highlighted general associations but have not fully explored this dynamic in Chattogram City Corporation.
Therefore, this cross-sectional study aims to determine the prevalence of diarrhea among under-five children in Chattogram City Corporation and to assess the WASH practices of their mothers. It further seeks to examine the association between maternal WASH practices and the occurrence of diarrheal disease in their children. By generating localized evidence, this study seeks to inform context-specific public health strategies to reduce the diarrheal burden in this rapidly growing urban setting.
2.1. Study design and setting
A community-based, cross-sectional study was conducted from March to September 2022 within the Chattogram City Corporation, Bangladesh. The study population comprised mothers of children under five years of age, attending OPD of two tertiary-level hospitals in Chattogram. A probability proportional to size (PPS) sampling method was subsequently employed to account for disparities in child population density across different locations, thereby enhancing the representativeness of the sample [20]
2.2. Sample size calculation
The minimum sample size was calculated using the single population proportion formula:

where, n = number of samples.
z = 1.96 (95% confidence level);
p= 0.11 [21]
q=(1-p); and
d = Precision of the prevalence estimate (0.05).

This estimated a minimum sample of 150. To account for potential non-response and incomplete data, the sample was increased by 20%, resulting in a final target of 182 participants. From the PPS-derived sampling frame, participants were selected using a simple random sampling method from mothers of children under five years of age attending OPD of two tertiary-level hospitals in Chattogram: 98 participated from Maa-o-Shishu Hospital, and the remaining 84 participated from Bangabandhu Memorial Hospital.
2.3. Data collection tool
Data was collected using a pre-tested, semi-structured questionnaire adapted from relevant previous studies [21, 22]. The instrument was prepared in both English and Bengali and covered key domains: socio-demographic characteristics, household water sources and storage practices, water treatment methods, sanitation and hygiene practices, and the occurrence, clinical features, and management of diarrheal episodes in the index child. The Bengali version was pre-tested (not included in the final sample) on 15 mothers (10%) to assess question clarity, acceptability, and flow, then adjusted according to the pre-test. The questionnaire was reviewed and finalized by an interdisciplinary team of epidemiologists and public health experts during ethical approval, and suggested changes were adapted in the questionnaire.
2.4. Variables and conceptual framework
The primary outcomes were the occurrence and frequency of diarrheal episodes among children younger than five years, together with treatment-seeking behaviors and antibiotic use. The conceptual framework (Figure 1) illustrates diarrheal infection as the central outcome influenced by four interrelated domains: socio-demographic characteristics, household WASH infrastructure, maternal WASH practices, and diarrhea management, including antibiotic use. Socio-demographic factors like child age, maternal occupation, and household income serve as distal determinants influencing two interrelated streams: urban infrastructure determinants (toilet type, sewage availability, water sources, and flooding) and maternal WASH practices (hand hygiene, water practices, and sanitation maintenance). Both streams directly influence diarrheal occurrence, frequency, and duration among under-five children. The framework further positions treatment and antibiotic misuse as a critical parallel pathway: diarrheal episodes trigger treatment responses, but the widespread practice of combining antibiotics with oral saline often inappropriately creates dual challenges of inadequate case management and antimicrobial resistance. Key pathways include effects of infrastructure and behaviors on diarrhea, infrastructure enabling or constraining behaviors, and the response pathway from diarrhea to antibiotic misuse, contributing to a broader public health burden. This framework guided the analytical approach examining associations between WASH variables and diarrheal outcomes, with parallel consideration of treatment patterns.
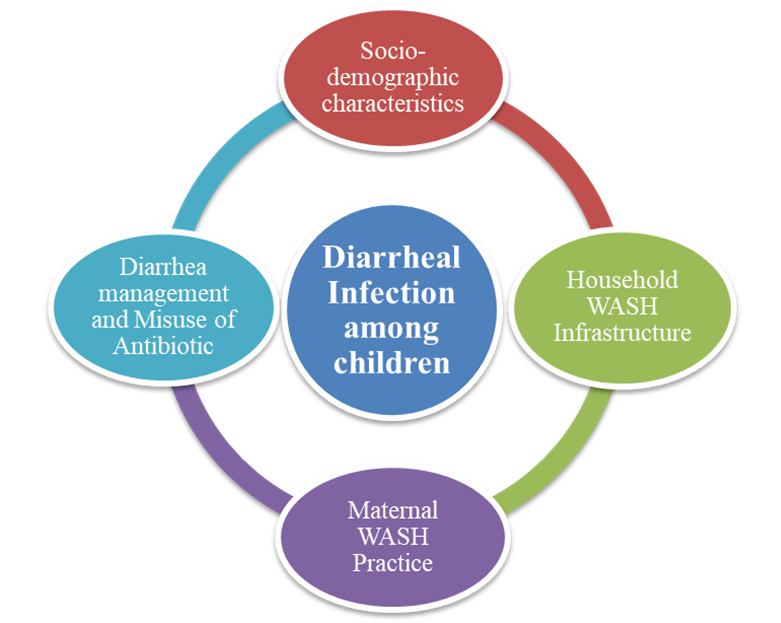
Figure 1. Conceptual Framework of this study.
2.5. Data analysis
Data were analyzed using IBM SPSS Statistics (Version 22). Descriptive statistics were computed for all variables. Associations between categorical WASH variables and diarrheal outcomes were assessed using the Chi-square test, and regression model analysis with a statistical significance level set at p <0.05. The manuscript was prepared in accordance with the STROBE checklist for cross-sectional studies.
3.1. Socio-demographic characteristics
A total of 182 mother-child dyads were included in the analysis. As shown in Table 1, the age distribution of the children showed that the 49 to 59 months-older group constituted the largest group (34.6%), while less than 12 months and 12 to 24 months old were the smallest (12.6% and 12.1%). Children aged 37 to 48 months comprised 17.6% of the sample. Regarding maternal occupation, 53.0% were homemakers and 33.0% were labor-based workers. Most families (65.9%) reported a monthly income of less than 20,000 BDT, while 23.1% earned between 21,000 and 30,000 BDT, while the mean monthly family income of the respondents was 24035 BDT.
Table 1. Socio-demographic characteristics of the participants.
| Variables | Frequency (n) | Percentage (%) |
| Age of Children in months (Mean ± SD = 29.52 ± 7.41) | ||
| Less than 12 months | 23 | 12.6 |
| 13 to 24 months | 22 | 12.1 |
| 25 to 36 months | 42 | 23.1 |
| 37 to 48 months | 32 | 17.6 |
| 49 to 59 months | 63 | 34.6 |
| Mother Occupation | ||
| Housewife | 97 | 53.0 |
| Private Job | 16 | 9.0 |
| Self Employed | 9 | 5.0 |
| Labor-based worker | 60 | 33.0 |
| Monthly Family Income in BDT (Mean ± SD = 24035 ± 13000.45) | ||
| Less than 20000 | 120 | 65.9 |
| 21000-30000 | 42 | 23.1 |
| 31000-40000 | 16 | 8.8 |
| 41000-50000 | 4 | 2.2 |
3.2. Prevalence of Diarrheal disease
Table 2 shows mothers reported that 69.2% of children had experienced a diarrheal episode within the last 5 months, 11.0% between 5 to 11 months ago, and 19.8% more than 11 months ago. In the preceding 12 months, 48.4% of children experienced 1-2 diarrheal episodes, 35.2% experienced 3-4 episodes, and 2.2% had more than four episodes; 14.3% had no diarrhea. The duration of illness was less than 4 days for 51.6% of children, 4-6 days for 37.4%, and more than 6 days for 11.0%. Regarding treatment, 9.9% of mothers used no formal treatment, 33.0% visited a local pharmacy, 34.1% sought medical advice, and 23.1% hospitalized their child. During episodes, 71.4% of mothers administered both antibiotics and oral saline, 12.1% gave oral and rice saline, 9.9% provided natural fruit juices, 5.5% gave only oral saline, and 1.1% provided none. For feeding during illness, 59.3% of mothers offered soup/liquid food, 28.6% provided cooked rice and curry, and 12.1% offered various foods.
Table 2. Characteristics of diarrheal prevalence and treatment strategies.
| Variables | Frequency | Percent (%) |
| Last diarrheal infection | ||
| Less than 5 Month | 126 | 69.2 |
| 5 to 11 Month | 20 | 11.0 |
| 12 Month or More | 36 | 19.8 |
| Diarrheal count in 12 months (Mean ± SD = 2.02 ± 1.35) | ||
| Never | 26 | 14.3 |
| 1-2 times | 88 | 48.4 |
| 3-4 times | 64 | 35.2 |
| More than 4 times | 4 | 2.2 |
| Duration of Infection | ||
| Less than 4 Day | 94 | 51.6 |
| 4 to 6 Day | 68 | 37.4 |
| More than 6 Day | 20 | 11.0 |
| Source of treatment | ||
| None | 18 | 9.9 |
| Local Medicine Shop | 60 | 33.0 |
| Doctor or Health Worker | 62 | 34.1 |
| Hospital Admission | 42 | 23.1 |
| Given type of medicine during the last infection | ||
| Only Oral Saline | 10 | 5.5 |
| Both Oral and Rice Saline | 22 | 12.1 |
| Antibiotic and Oral Saline | 130 | 71.4 |
| Natural Fruit Juice | 18 | 9.9 |
| None | 2 | 1.1 |
| Type of Food during the last infection | ||
| Soup or Liquid Food | 108 | 59.3 |
| Cooked Rice and Curry | 50 | 27.5 |
| Other’s | 24 | 13.2 |
3.3. Sanitation facilities and associated factors
Table 3 presents the association between household sanitation practices and the frequency of diarrheal episodes among under-five children. Half of the households (50.5%) used a pit latrine with a sewage channel, 37.4% used a toilet with ideal sanitary facilities, 9.9% used a pit latrine without a channel, and 2.2% used other types. The number of users per toilet was fewer than 5 in 53.8% of households, 5-8 in 34.1%, and more than 8 in 12.1%. Toilet cleaning frequency was twice weekly for 45.1% of households, once weekly for 34.1%, three or more times weekly for 18.7%, and never for 2.2%. Mothers graded toilet cleanliness as moderate/good (47.3%) or bad (4.4%); the remainder did not specify. A sewage channel was present in the washroom for 72.5% of households and absent for 27.5%. A majority (56.0%) reported being affected by flood/waterlogging during the rainy season. Statistical analysis revealed significant associations between diarrheal episode count in the last 12 months and several sanitation variables: toilet cleanliness grade (P=0.007), type of toilet used (P=0.024), toilet cleaning frequency (P=0.014), and availability of a sewage channel (P=0.012). No significant association was found with the number of toilet users (P=0.125), place of taking baths (P=0.690), or flood/waterlogging record (P=0.574).
Table 3. Association between sanitation practice and diarrheal infection in last 12 months.
| Variables | Diarrheal count in last 12 months | Total | Percent (%) | P-Value | |||
| Never | 1-2 times | 3-4 times | More than 4 times | ||||
| Toilet type | |||||||
| Pit Latrine Without Sewage Channel | 0 | 8 | 8 | 2 | 18 | 9.9 |
0.024 |
| Pit Latrine with Sewage Channel | 14 | 32 | 46 | 0 | 92 | 50.5 | |
| Toilet with Ideal Sanitary Facilities | 12 | 46 | 8 | 2 | 68 | 37.4 | |
| Other’s | 0 | 2 | 2 | 0 | 4 | 2.2 | |
| Number of single toilet user | |||||||
| Less than 5 | 22 | 44 | 30 | 2 | 98 | 53.8 |
0.125 |
| 5 to 8 | 2 | 36 | 24 | 0 | 62 | 34.1 | |
| More than 8 | 2 | 8 | 10 | 2 | 22 | 12.1 | |
| Toilet cleaning frequency per week | |||||||
| Never | 0 | 0 | 4 | 0 | 4 | 2.2 |
0.014 |
| Once | 2 | 22 | 34 | 4 | 62 | 34.1 | |
| Twice | 20 | 46 | 16 | 0 | 82 | 45.1 | |
| Thrice | 4 | 8 | 8 | 0 | 20 | 11.0 | |
| More than thrice | 0 | 12 | 2 | 0 | 14 | 7.7 | |
| Toilet cleanliness management | |||||||
| Bad | 0 | 0 | 6 | 2 | 8 | 4.4 |
0.007 |
| Moderate | 10 | 40 | 36 | 0 | 86 | 47.3 | |
| Good | 16 | 48 | 22 | 2 | 88 | 48.4 | |
| Place of taking bath | |||||||
| Washroom | 26 | 82 | 58 | 4 | 170 | 93.4 |
0.690 |
| Open Space | 0 | 6 | 6 | 0 | 12 | 6.6 | |
| Sewage channel connection with toilet | |||||||
| Yes | 22 | 72 | 38 | 0 | 132 | 72.5 | 0.012 |
| No | 4 | 16 | 26 | 4 | 50 | 27.5 | |
| Flood and water logging around home in rainy season | |||||||
| Yes | 12 | 46 | 42 | 2 | 102 | 56.0 |
0.574 |
| No | 14 | 42 | 22 | 2 | 80 | 44.0 | |
3.4. Water source, storage, and hygiene
The primary drinking water source was a personal electrical water pump for 49.5% of households, WASA supply for 25.3%, tube wells for 22.0%, and deep tube wells for a smaller percentage (Table 4). Sources for cooking water were similar. Most children (53.8%) drank fewer than 4 glasses of water daily, 38.5% drank 4-6 glasses, and 7.7% drank more than 6 glasses. The majority (81.3%) were satisfied with their water source, while 12.1% were dissatisfied and 6.6% were highly satisfied. Most households (71.4%) had a water reserve tank (51.6% rooftop plastic, 18.7% rooftop brick wall, and 1.1% subsurface), while 28.6% had none. Water purification before consumption was practiced in 58.2% of households and not practiced in 41.8%. No significant association was found between water purification practice and diarrheal count.
Table 4. Association between water consumption practices and diarrheal infection in the last 12 months.
| Variables | Diarrheal Count in Last 12 Months | Total | Percent (%) | P-Value | |||
| Never | 1-2 times | 3-4 times | More than 4 times | ||||
| Drinking water source | |||||||
| WASA | 6 | 28 | 12 | 0 | 46 | 25.3 | 0.149 |
| Tube-Well | 4 | 14 | 28 | 0 | 46 | 25.3 | |
| Personal Electrical Water Pump | 16 | 46 | 24 | 4 | 90 | 49.4 | |
| Kitchen water source | |||||||
| WASA | 6 | 28 | 12 | 0 | 46 | 25.3 | 0.202 |
| Tube-Well | 4 | 16 | 28 | 0 | 48 | 26.4 | |
| Personal Electrical Water Pump | 16 | 44 | 24 | 4 | 88 | 48.3 | |
| Glass of water drink everyday | |||||||
| Less than 4 Glass | 14 | 56 | 26 | 2 | 98 | 53.8 | 0.101 |
| 4 to 6 Glass | 12 | 26 | 32 | 0 | 70 | 38.5 | |
| More than 6 Glass | 0 | 6 | 6 | 2 | 14 | 7.7 | |
| Satisfaction on water sources | |||||||
| Not Satisfied | 2 | 6 | 14 | 0 | 22 | 12.1 | 0.354 |
| Satisfied | 20 | 76 | 48 | 4 | 148 | 81.3 | |
| Very Satisfied | 4 | 6 | 2 | 0 | 12 | 6.6 | |
| Water reservoir tank type | |||||||
| Underground Tank | 0 | 2 | 0 | 0 | 2 | 1.1 | 0.261 |
| Roof Top Plastic Tank | 14 | 50 | 26 | 4 | 94 | 51.6 | |
| Rooftop Brick-Wall Tank | 8 | 18 | 8 | 0 | 34 | 18.7 | |
| None | 4 | 18 | 30 | 0 | 52 | 28.6 | |
| Water purification method | |||||||
| Commercial or Pure-It Filter | 2 | 8 | 0 | 0 | 10 | 5.5 | 0.664 |
| Stone Based Layered Filter | 2 | 8 | 4 | 0 | 14 | 7.7 | |
| Boiled Water for 30 Minutes | 12 | 44 | 24 | 2 | 82 | 45.0 | |
| No Filtration | 10 | 28 | 36 | 2 | 76 | 41.8 | |
3.5. Hand and food hygiene practices
As shown in Table 5, most of the mothers (89.0%) reported always washing hands before/after eating and before feeding children, while 11.0% did so occasionally. After defecation, 68.1% always washed hands and 31.9% did so occasionally. For produce washing, 42.9% always washed fruits/vegetables before consumption/cooking, 49.5% did so sometimes, and 7.7% never did. Handwashing agents included bar soap (53.8%), liquid soap (39.6%), ashes/alternatives (3.3%), and nothing (3.3%). Significant associations with diarrheal episode count were found for washing hands after defecation (P=0.002), washing produce before eating/cooking (P=0.000), washing hands before/after food consumption (P=0.012), and the type of soap used for handwashing (P=0.017).
Table 5. Association between hygiene practices and diarrheal infection count in last 12 months.
| Characteristics | Diarrheal count in last 12 months | Total | Percent (%) | P-Value | |||
| Never | 1-2 times | 3-4 times | More than 4 times | ||||
| Wash Hands after using the Washroom | |||||||
| Sometimes | 0 | 2 | 16 | 2 | 20 | 11.0 | 0.002 |
| Every time | 26 | 86 | 48 | 2 | 162 | 89.0 | |
| Wash Hands before and after consuming food | |||||||
| Sometimes | 4 | 20 | 30 | 4 | 58 | 31.9 | 0.012 |
| Every time | 22 | 68 | 34 | 0 | 124 | 68.1 | |
| Wash fruit/vegetable before eat/cook | |||||||
| Never | 0 | 0 | 10 | 4 | 14 | 7.7 | 0.000 |
| Sometimes | 6 | 34 | 38 | 0 | 78 | 42.9 | |
| Every time | 20 | 54 | 16 | 0 | 90 | 49.4 | |
| Types of soap uses to wash hands | |||||||
| None | 0 | 2 | 4 | 0 | 6 | 3.3 | 0.017 |
| Bar soap | 12 | 50 | 36 | 0 | 98 | 53.8 | |
| Liquid Soap | 14 | 36 | 20 | 2 | 72 | 39.6 | |
| Other’s | 0 | 0 | 4 | 2 | 6 | 3.3 | |
Table 6 summarizes the results of the multiple linear regression analysis examining the association between WASH-related factors and the frequency of diarrheal episodes. The regression model demonstrated a moderate positive correlation (R = 0.549) between the predictor variables and diarrheal frequency, explaining 30.2% of the variance (R² = 0.302). The adjusted R² of 0.214 indicates that after accounting for the number of predictors, approximately 21.4% of the variance in diarrhea frequency is explained by the model. The model was statistically significant (F = 3.454, p = 0.001), indicating that the set of WASH-related predictors reliably predicts diarrheal frequency.
None of the individual predictors reached conventional statistical significance at the α = 0.05 level. However, three variables demonstrated marginally significant associations with diarrheal frequency. Toilet cleaning frequency showed a negative association approaching significance (B = -0.288, β = -0.196, t = -1.839, p = 0.070, 95% CI: -0.600 to 0.024), suggesting a trend toward fewer diarrhea episodes with more frequent toilet cleaning. Presence of Sewerage Channel Attached to Washroom exhibited a positive association approaching significance (B = 0.612, β = 0.204, t = 1.953, p = 0.054, 95% CI: -0.012 to 1.237), counterintuitively suggesting a trend toward higher diarrhea frequency in households with sewerage connections. Handwashing before and after food consumption demonstrated a negative association approaching significance (B = -0.888, β = -0.207, t = -1.843, p = 0.069, 95% CI: -1.848 to 0.071), indicating a trend toward fewer diarrhea episodes with proper handwashing practices.
Table 6. Linear regression model of the association of frequency of having diarrhea in the past 12 months among children with wash practice.
| Model Summary | ||||||||||||||
| R | R Square | Adjusted R square | Std. Error of the Estimate | Change Statistics | ||||||||||
| R Square change | F Change | df1 | df2 | Sig. F change | ||||||||||
| 0.549 | 0.302 | 0.214 | 1.196 | 0.302 | 3.454 | 10 | 80 | 0.001 | ||||||
| Coefficients a | ||||||||||||||
| Unstandardized coefficients | Standardized coefficients | t | Sig. | 95.0% confidence interval for B | Correlations | Collinearity statistics | ||||||||
| B | Std. Error | Beta | Lower Bound | Upper Bound | Zero order | Partial | Part | Tolerance | VIF | |||||
| (Constant) | 6.091 | 1.839 | 3.311 | .001 | 2.430 | 9.751 | ||||||||
| Children age in months | .038 | .095 | .039 | .397 | .692 | -.152 | .227 | .071 | .044 | .037 | .905 | 1.105 | ||
| Mothers’ Education | -.013 | .168 | -.010 | -.080 | .937 | -.347 | .320 | -.271 | -.009 | -.007 | .530 | 1.886 | ||
| Mothers’ Occupation | .037 | .066 | .063 | .559 | .578 | -.094 | .168 | .117 | .062 | .052 | .684 | 1.463 | ||
| Monthly family income | .007 | .191 | .004 | .036 | .972 | -.372 | .386 | -.134 | .004 | .003 | .695 | 1.440 | ||
| Frequency of cleaning toilet per week | -.288 | .157 | -.196 | -1.839 | .070 | -.600 | .024 | -.348 | -.201 | -.172 | .770 | 1.299 | ||
| Cleanliness and Environment of toilet | -.150 | .273 | -.065 | -.551 | .583 | -.693 | .393 | -.296 | -.061 | -.051 | .632 | 1.582 | ||
| Sewerage channel attached with toilet | .612 | .314 | .204 | 1.953 | .054 | -.012 | 1.237 | .338 | .213 | .182 | .802 | 1.246 | ||
| Wash hand before and after eating | -.888 | .482 | -.207 | -1.843 | .069 | -1.848 | .071 | -.387 | -.202 | -.172 | .692 | 1.445 | ||
| Wash hand after using toilet | -.471 | .359 | -.164 | -1.314 | .193 | -1.185 | .243 | -.323 | -.145 | -.123 | .563 | 1.776 | ||
| Type of hand-washing material | -.015 | .235 | -.007 | -.065 | .948 | -.484 | .453 | -.011 | -.007 | -.006 | .754 | 1.327 | ||
a Dependent Variable: Frequency of having Diarrhea in past 12 months among children.
Child age (p = 0.692), mother's educational qualification (p = 0.937), mother's occupation (p = 0.578), monthly family income (p = 0.972), grading of toilet cleanliness (p = 0.583), handwashing after using the washroom (p = 0.193), and type of handwashing material (p=0.948) were not statistically significant predictors of diarrheal frequency. Variance Inflation Factor (VIF) values ranged from 1.105 to 1.886, all well below the conventional threshold of 10, indicating no significant multicollinearity among the predictor variables. Tolerance statistics ranged from 0.530 to 0.905, further supporting the absence of problematic multicollinearity. Zero-order correlations revealed that toilet cleaning frequency (r = -0.348), handwashing practices (r = -0.387 for food-related and r = -0.323 for toilet-related), and sewerage attachment (r = 0.338) showed the strongest bivariate associations with diarrhea frequency, consistent with their marginally significant status in the multivariable model. The model suggests that while the overall set of WASH practices significantly predicts diarrhea frequency, the individual contributions of specific practices do not achieve statistical significance at the conventional level, possibly due to sample size limitations or shared variance among predictors.
The present study aimed to contribute to a nuanced understanding of the persistent burden of childhood diarrhea and the complex interplay of associated and non-associated WASH behaviors in this urban context. The high recent prevalence of diarrhea reported among study children (69.2% within the last five months) aligns with and exceeds the national estimate of 46.7% [17], reflecting the significant local disease burden. The reported episode frequency, where 35.2% of children experienced 3-4 episodes in the last year, corresponds with previous estimates from Bangladesh [23]. While most mothers sought treatment from formal or informal sources, the 9.9% who did not seek any treatment, though lower than global (56%) and regional (>40%) averages [24, 25], remains a critical concern for child health outcomes. Regarding case management, the predominant use of both antibiotics and oral saline (71.4%) indicates a common, yet problematic, treatment approach. This aligns with findings that while mothers recognize oral rehydration therapy (ORT) for fluid replacement, its perceived inability to "cure" diarrhea drives concurrent antibiotic use [26–29]. The high co-administration of antibiotics with oral rehydration saline suggests limited awareness of prudent antibiotic practices, aligning with similar high misuse rates documented in prior studies [30–32]. This practice underscores the need for education on the appropriate use of ORT and the risks of antibiotic misuse.
In addition, no significant association between water consumption practices and diarrheal episodes in the last 12 months. Specifically, variables such as drinking water source, kitchen water source, daily glasses of water consumed, satisfaction with water sources, water reservoir tank type, and water purification method showed no significant relation with diarrheal count. This contrasts with some previous studies that identified contributing water-related factors to diarrhea [33]. However, concerning water practices, a substantial proportion of households (41.8%) did not purify their drinking water. This contrasts with a previous Chattogram study where boiling and filtration were more commonly reported [34, 35] and highlights a crucial gap in point-of-use water safety management, which is a known risk factor for diarrhea [14]. The lack of statistical association despite this gap may suggest that other transmission pathways, particularly poor sanitation and hygiene, exert a more dominant influence in this setting.
Moreover, this study reveals significant associations between diarrheal frequency and toilet cleanliness, type of toilet used, cleaning frequency, and sewage channel availability. This corroborates evidence that improved sanitation reduces childhood diarrhea [22]. Furthermore, the presence of a sewerage channel attached to the toilet showed a positive association with diarrhea frequency, which may indicate the influence of sanitary infrastructure and waste disposal systems on environmental pollution and the spread of diarrheal diseases [36, 37]. It is suggested that the potential advantages of toilet type may be restricted in the absence of consistent sanitation practices.
The lack of association with flooding/waterlogging is notable, suggesting other immediate WASH factors may exert a stronger influence on transmission in this setting. As the study showed, more frequent toilet cleaning and proper handwashing practices suggested a trend toward fewer diarrheal episodes, with some variables demonstrating borderline significance. These findings demonstrate concordance with earlier studies reporting that proper sanitation and hygiene practices significantly reduce diarrhea [38, 39].
Our results strongly reinforce the critical role of hygiene behaviors. The regression model suggests that while the overall set of WASH practices significantly (R = 0.549) predicts diarrhea frequency, the individual contributions of specific practices do not achieve statistical significance at the conventional level, possibly due to sample size limitations or shared variance among predictors. We found significant correlations between diarrheal frequency and key practices: washing produce before eating/cooking, handwashing after defecation, handwashing before/after food consumption, and the type of handwashing agent used. This aligns with the established framework of WASH-related risk factors [40] and specific evidence linking poor handwashing to acute diarrhea [15]. While almost full proportion of post-defecation handwashing in the study contrasts with findings of another study of only 3.1% non-compliance, the persistent association emphasizes that consistency and technique, particularly the use of soap, are as vital as the practice itself [41]. The significant association between handwashing agent type and diarrheal frequency underscores that the quality of hand hygiene, not merely its occurrence, determines its protective effect.
Overall, this study identifies that while water-related practices showed no significant association with diarrhea among children under-5 in this Chattogram setting, sanitation infrastructure and hygiene behaviors emerged as critical determinants. The widespread antibiotic misuse (71.4%) represents a parallel public health crisis requiring urgent intervention. To effectively reduce the diarrheal burden, public health interventions must prioritize sustained behavior change in hygiene practices and sanitation maintenance alongside infrastructure improvements, while concurrently addressing antibiotic misuse through targeted education on appropriate ORT use.
The study limited itself to the Bangladeshi district of Chittagong. Because of this, it's possible that the results cannot be applied to the whole population of children under five years in the nation. The data was self-reported and collected information from the past 12 months, which may cause recall bias. Since the research strategy used in this study was cross-sectional, it is not possible to infer causality from the relationships found. Additionally, the statistical power and consistency of the study's conclusions are constrained by the small sample size. The small sample size may have limited the statistical ability to find significant relationships between particular WASH factors and frequency of diarrheal event. Furthermore, the regression model explained only a significant fraction of variation, indicating that other unmeasured variables may impact outcomes. Moreover, the tight time schedule and lower budget are issues that influence the study.
In conclusion, this study identifies several modifiable WASH practices, particularly related to hand hygiene, food washing, toilet maintenance, and point-of-use water treatment, that are significantly associated with diarrheal disease prevalence among young children in Chattogram. Although no individual predictors emerged independently, the findings showed WASH practices had a combined effect on diarrheal incidence among under-five children. Public health efforts may benefit from approaches that extend beyond infrastructure development, potentially incorporating strategies that support long-term behavioral shifts. Health education directed at mothers could highlight practices such as regular handwashing with soap at key moments, maintaining food hygiene, and preparing and using oral rehydration therapy appropriately. These behavioral components might be considered alongside ongoing initiatives aimed at improving access to safe water and sanitation, contributing to broader efforts to address childhood diarrheal morbidity.
The authors gratefully acknowledge the contributions of all co-authors to the conceptualization, analysis, and preparation of this study. Thankful to the authority of university for supporting to conduct this study. The authors also note that limited AI-assisted tools (about 11%) were used primarily for language editing and creating diagram, in accordance with the journal’s editorial policy.
The study was conducted to fulfill an academic purpose. There were no funding sources available for this study.
The authors declare no competing interests.
This study did not involve any experiments on human participants or animals. Ethical approval was obtained from the Research Ethics Committee of the Faculty of Allied Health Sciences, Daffodil International University (Reference no. FAHS-REC/2022/028). Prior to data collection, the study's purpose, procedures, and data privacy policies were explained to all potential participants. Written informed consent was obtained from each respondent. All collected information was kept strictly confidential and anonymized during analysis.

This work is licensed under a
Creative Commons Attribution 4.0 International License
.
You are free to share and adapt this material for any purpose, even commercially, as long as you give appropriate credit.
 access
access