J. Biosci. Public Health. 2026; 2(3)
First and Corresponding Author
![]() https://orcid.org/0009-0004-9615-3729
https://orcid.org/0009-0004-9615-3729
Affiliations:
Department of Public Health and Informatics, Jahangirnagar University, Dhaka-1342, Bangladesh
Coauthor
![]() https://orcid.org/0009-0000-6913-2595
https://orcid.org/0009-0000-6913-2595
Affiliations:
Department of Public Health and Informatics, Jahangirnagar University, Dhaka-1342, Bangladesh
Coauthor
raiyaantabassumimita@gmail.com
![]() https://orcid.org/0009-0005-5945-1919
https://orcid.org/0009-0005-5945-1919
Affiliations:
Department of Public Health and Informatics, Jahangirnagar University, Dhaka-1342, Bangladesh
Coauthor
![]() https://orcid.org/0000-0001-8421-517X
https://orcid.org/0000-0001-8421-517X
Affiliations:
Department of Public Health and Informatics, Jahangirnagar University, Dhaka-1342, Bangladesh
Coauthor
![]() https://orcid.org/0000-0002-7186-7774
https://orcid.org/0000-0002-7186-7774
Affiliations:
Department of Public Health and Informatics, Jahangirnagar University, Dhaka-1342, Bangladesh
Background: Menstrual hygiene management remains a critical yet underexplored public health issue in Bangladesh, particularly regarding how different menstrual materials shape women’s needs and insecurities. This study examined differences in menstrual needs and insecurities between female university students in Bangladesh who use disposable and reusable menstrual products. Methods: A cross-sectional survey was conducted among 625 female university students from five administrative divisions of Bangladesh between January and February 2024. Data were collected using a structured questionnaire of the Menstrual Practice Needs Scale (MPNS-36). Multivariate linear regression analyses were performed. Results: Although overall menstrual needs scores did not differ significantly at the unadjusted level, multivariate analyses revealed that reusable menstrual material users experienced significantly poorer outcomes across several domains. The reusable material users reported significantly lower scores for material and home environment needs (β = −0.21, 95% CI: −0.34, −0.09; p = 0.001), transport and university environment needs (β = −0.18, 95% CI: −0.30 to −0.05; p = 0.006), reuse needs (β = −0.23, 95% CI: −0.39, −0.06; p = 0.007), and overall menstrual needs (β = −0.12, 95% CI: −0.20, −0.03; p = 0.010). However, no significant differences were observed for material reliability concerns, change and disposal, or reuse insecurity. Conclusion: Reusable menstrual material use was associated with poorer menstrual needs experiences in key environmental and practical domains among university women in Bangladesh. These findings highlight the need for context-specific interventions that address infrastructural barriers, ensure adequate facilities, and support safe and dignified use of reusable menstrual products.
Menstruation remains a significant yet often overlooked aspect of reproductive health for young women, influencing their physical well-being, educational opportunities, and social engagement across diverse contexts. Inadequate menstrual hygiene practices contribute to health complications such as reproductive tract infections, alongside disruptions in daily activities like schooling and work [1,2]. These challenges are compounded by the limited availability of facilities. Worldwide, nearly 1.8 billion individuals experience menstruation each month, but access to safe and effective management remains remarkably inadequate, with around 500 million lacking adequate access to products and facilities for safe management. The situation is particularly exacerbated in low- and middle-income countries [3]. In South Asia, including Bangladesh, menstrual hygiene management (MHM) often hinges on the choice between disposable and reusable materials, each carrying distinct implications for health, affordability, and environmental sustainability [4]. While disposable pads offer convenience and perceived hygiene, these may pose environmental concerns due to non-biodegradability and can be highly expensive for many households [5]. Reusable options, such as cloths or fabric pads, provide a cost-effective alternative but require proper cleaning and drying to prevent infections, which is frequently hindered by taboos that discourage open drying or washing [6, 7]. Cultural norms in these areas frequently view menstruation as impure, leading to restrictions on mobility, religious participation, and even dietary habits during periods [8].
In Bangladesh, a densely populated nation with over 170 million people, MHM poses tremendous challenges, particularly among adolescents and young women who constitute a significant demographic. Traditional methods, such as reused cloths, dominate usage, with only about 24% of reproductive-age women employing modern disposable absorbents like sanitary pads, a figure that drops markedly in rural and low-income settings [9]. Among adolescent girls in schools, this figure is more notable, with 86% using cloths and just 10% opting for pads, influenced heavily by urban-rural divides. In urban slums, usage shifts slightly, with half of women and girls employing pads, yet cloth remains prevalent at 42%, driven by factors like home accessibility and almost zero cost [8]. However, such practices often lead to insecurities, including fears of leakage, bad smell, or staining, which contribute to social isolation and stigma, affecting 41% of schoolgirls for an average of 2.8 days per cycle. Furthermore, 70% of rural women use cloths, but only a fraction adheres to hygienic drying in sunlight due to social taboos [8, 10].
Determinants of material choice in Bangladesh include socioeconomic status, education, and media exposure. Higher education levels and urban households correlate with greater pad adoption. Additionally, embarrassment in purchasing pads from male vendors is also a great deterrent [9]. Despite growing attention to menstrual health globally, research on preferences between disposable and reusable materials remains underexplored, especially in Bangladesh, where local contexts, such as cultural norms and economic constraints, shape usage patterns. Few studies looked into the specific needs and insecurities of young women, overlooking how stigma or infrastructure gaps hinder shifts from traditional clothes to sustainable options. This gap limits the development of evidence-based policies, underscoring the urgency. This study examines needs, insecurities, and determinants shaping disposable versus reusable menstrual material preferences among young Bangladeshi women. By elucidating these patterns through empirical inquiry, it aims to inform targeted interventions that enhance MHM equity, aligning with Sustainable Development Goals (SDG) on health and sanitation.
2.1. Study design, setting, and population
A nationally representative cross-sectional survey was conducted from January to February 2024 among female university students throughout Bangladesh. Data were collected from five universities, each situated in a distinct administrative division of the country. The study population comprised female students enrolled in Bangladeshi universities who had attained menarche at least two years prior to data collection and reported having either regular or irregular menstrual cycles. Students who had not yet reached menarche or declined to provide informed consent were excluded. Furthermore, individuals with serious medical conditions that could influence menstruation, such as hysterectomy or hormonal disorders, were deemed ineligible for participation.
2.2. Sample size and technique
The minimum required sample size was calculated using the following Cochran’s formula for sample size estimation in a cross-sectional study [11, 12].


A conservative prevalence estimate of 0.50 was adopted in the sample size calculation to maximize variability, as is standard practice in this context. For multi-stage sampling designs, a margin of error of 5% and a design effect of 1.5 are typically applied [13]. Based on these parameters, the initial minimum sample size required for this study was calculated to be 576 participants. However, we exceeded the sample size and included a total of 625 participants for the final analysis, which was then distributed equally among the 5 universities.
A multistage sampling method was used to recruit participants for the study (Figure 1). The eight administrative divisions of Bangladesh served as the primary clusters, while universities within each division constituted the secondary clusters. In the first stage, five divisions, Dhaka, Rajshahi, Chittagong, Sylhet, and Khulna, were randomly selected.
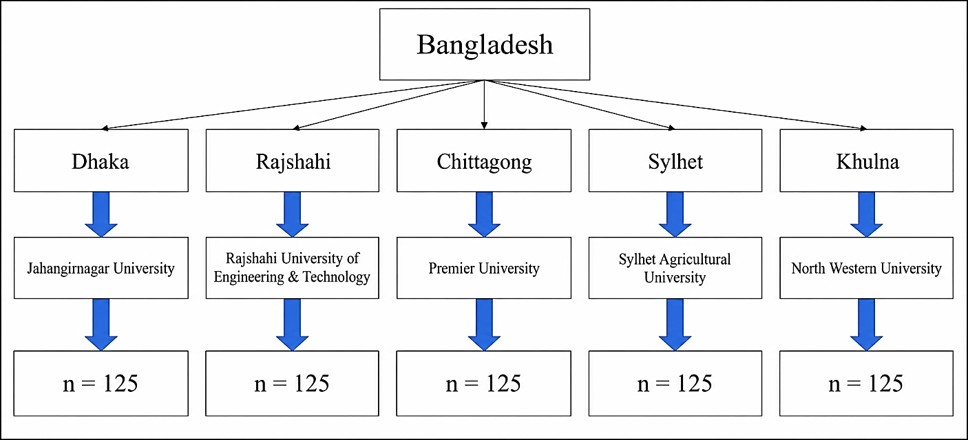
Figure 1. Sampling framework for the study.
Subsequently, one university was randomly chosen from each selected division, leading to the inclusion of five universities in total. In the final stage, an equal number of students (n = 125) were selected from each university using consecutive sampling, ensuring comparable representation across the participating institutions. Participant recruitment was conducted consecutively within each selected university and continued until the predetermined sample size (n = 625) was reached. Students who refused participation or withdrew before survey completion were substituted with other eligible participants from the same institution. Consequently, the final analytical sample consisted of 625 completed questionnaires, ensuring that losses due to non-response or withdrawal did not affect the target sample size. Equal allocation of participants (n = 125) per university was intentionally adopted to ensure balanced representation across geographically diverse institutions and to facilitate meaningful comparisons between universities. Given the substantial variation in student enrollment across universities, proportional allocation would have resulted in the overrepresentation of larger institutions and limited the representation of smaller universities. Therefore, equal allocation was considered more appropriate for achieving comparable estimates across study sites.
Although the sampling process involved clustering at the university level, the study’s primary objective was to estimate the overall prevalence and examine associations at the individual level rather than generate university-specific estimates. In addition, the number of clusters was limited (five universities), and the analysis focused on pooled individual-level data; clustering was not explicitly modeled in the final analyses; however, this limitation has been acknowledged in the manuscript.
2.3. Survey instrument and data collection
Data were collected through face-to-face interviews while maintaining participant confidentiality, using a structured, interviewer-administered questionnaire conducted in Bengali to ensure clarity and accurate responses. No personally identifying information, such as names, student identification numbers, telephone numbers, or addresses, was recorded in the study database. All responses were coded using unique identification numbers and analyzed in de-identified form. The validated Bengali version of the Menstrual Practice Needs Scale (MPNS-36), translated by the official Menstrual Health Evidence Group, was used for this purpose [11,14]. This has allowed the interviewers to collect data in their native language, reducing potential biases. The questionnaire consisted of two sections. The first captured socio-demographic information, adapted from previous studies on menstrual practices and needs [15, 16]. The second included the MPNS-36, a validated instrument measuring unmet menstrual needs using 4-point Likert-scale items (Never to Always), which has demonstrated good reliability and validity in earlier studies [17]. To reduce reporting and social desirability bias, data were collected confidentially in private settings by trained female interviewers, and participants were assured of confidentiality. Their training covered the study objectives, participant recruitment procedures, informed consent process, questionnaire administration, ethical considerations, confidentiality protection, and techniques for conducting interviews on sensitive topics. Mock interviews and pilot testing sessions were also conducted to ensure consistency and standardization across interviewers. Random recruitment across university departments was used to minimize selection bias.
2.4. Statistical analysis
Field data were initially entered into Microsoft Excel 2021, where preliminary preprocessing, including coding and score calculation, was performed. Subsequent analyses were conducted in RStudio (Version 2024.12.0+467) using R (version 4.2.1). The tidy verse, gtsummary, and gt packages were applied for statistical analyses and generating publication-quality tables, while ggplot2 and ggpubr were used for data visualization. Descriptive statistics summarized categorical variables as frequencies and percentages, and continuous variables as mean ± standard deviation. Multiple linear regression was employed to association between unmet menstrual needs and types of menstrual management materials. Before conducting multiple linear regression, the underlying assumptions were evaluated and found to be adequately satisfied. Homoscedasticity was assessed by plotting standardized residuals against fitted values and showed no substantial evidence of heteroscedasticity. Multicollinearity was evaluated using variance inflation factors (VIFs), with values ranging from 1.12 to 2.84, well below the recommended threshold of 5.0. The independence of residuals was confirmed using the Durbin-Watson statistic (DW = 1.98), indicating no significant autocorrelation. Furthermore, Cook’s distance values were all below 0.50, suggesting the absence of influential observations. Overall, the regression model demonstrated a satisfactory fit to the data (F = 15.72, p < 0.001), explaining 31.4% of the variance in the outcome variable (Adjusted R² = 0.314). Statistical significance was determined at a 95% confidence level with a p-value < 0.05.
2.5. Scoring and interpretation
Menstrual practice needs were assessed using the 36-item Menstrual Practice Needs Scale (MPNS-36) [17]. The MPNS-36 is designed to evaluate the extent to which menstrual management environments, resources, and experiences meet the needs of menstruating individuals across multiple domains, including access to menstrual materials, privacy, water and sanitation facilities, disposal options, comfort, and safety. Each item is rated on a four-point Likert scale reflecting the degree to which menstrual needs are met. Response options are scored from 0 to 3, with higher scores indicating that menstrual practice needs are better met. Negatively worded items are reverse coded before analysis to ensure that all items are oriented in the same direction. After recoding, item scores are summed and averaged to generate an overall MPNS-36 score, with possible values ranging from 0 to 3. In the present study, the MPNS-36 score was analyzed as a continuous variable, with higher values representing better menstrual practice experiences and greater fulfillment of menstrual health and hygiene needs.
Table 1 outlines the socio-demographic and menstrual profile of the 625 participants. Most participants were Muslim (86.0%), enrolled in the third academic year (33.0%), and resided in university halls (60.0%). Nearly half of the respondents came from urban areas (42.0%), while 31.0% and 27.0% were from rural and suburban areas, respectively. Approximately half of the fathers (49.0%) had completed graduation, whereas 30.0% of mothers were graduates. Fathers were predominantly engaged in service (42.0%) or business (40.0%), while the majority of mothers were housewives (75.0%). Most respondents belonged to nuclear families (84.0%), and the largest proportion reported a monthly family income of BDT 30,000–50,000 (38.0%).
Table 1. Sociodemographic characteristics and participants' general information (N = 625).
| Variable | Category | Frequency (n) | Percentage (%) |
| Age (years) | Mean ± SD | 22.12 ± 1.64 | — |
| Religion | Christian | 8 | 1.0 |
| Hindu | 79 | 13.0 | |
| Muslim | 538 | 86.0 | |
| Educational level | 1st year | 145 | 23.0 |
| 2nd year | 181 | 29.0 | |
| 3rd year | 206 | 33.0 | |
| 4th year | 59 | 9.5 | |
| Master's | 34 | 5.5 | |
| Residency | Hall | 372 | 60.0 |
| Home (with family) | 165 | 26.0 | |
| House beside campus | 88 | 14.0 | |
| Permanent residence | Rural | 196 | 31.0 |
| Sub-urban | 167 | 27.0 | |
| Urban | 262 | 42.0 | |
| Father's educational status | Illiterate | 10 | 1.6 |
| Primary | 44 | 7.4 | |
| Secondary | 134 | 21.0 | |
| Higher secondary | 133 | 21.0 | |
| Graduate | 304 | 49.0 | |
| Father's occupation | Business | 253 | 40.0 |
| Service | 260 | 42.0 | |
| Retired | 60 | 9.6 | |
| Others | 33 | 5.4 | |
| Unemployed | 19 | 3.0 | |
| Mother's educational status | Illiterate | 47 | 8.0 |
| Primary | 89 | 14.0 | |
| Secondary | 158 | 25.0 | |
| Higher secondary | 141 | 23.0 | |
| Graduate | 190 | 30.0 | |
| Mother's occupation | Housewife | 469 | 75.0 |
| Service | 133 | 21.0 | |
| Business | 2 | 0.3 | |
| Retired | 9 | 1.6 | |
| Unemployed | 12 | 2.1 | |
| Family structure | Nuclear | 524 | 84.0 |
| Extended | 101 | 16.0 | |
| Monthly family income (BDT) | <30,000 | 191 | 31.0 |
| 30,000–50,000 | 240 | 38.0 | |
| 50,000–70,000 | 119 | 19.0 | |
| >70,000 | 75 | 12.0 |
Regarding menstrual characteristics, 81.0% of participants had received information about menstruation before menarche (Table 2). The majority (73.0%) experienced menarche between 12 and 14 years of age. Most respondents (83.0%) reported normal menstrual bleeding during their most recent cycle. Menstrual complications were common, with 28.0% reporting oligomenorrhea, 28.0% multiple menstrual complications, 23.0% menorrhagia, and 21.0% polymenorrhea. More than half (56.0%) had a family history of dysmenorrhea, and 67.0% experienced severe menstrual pain. Most participants (68.0%) reported a menstrual duration of 3–5 days, while 42.0% used medication during menstruation. During menstruation, 46.0% consumed less food, 36.0% reported no change in food intake, and 18.0% consumed more food. Disposable menstrual products were used by 73.0% of participants, whereas 27.0% reported using reusable menstrual materials.
Table 2. Menstrual-related characteristics of the participants (N = 625).
| Variable | Category | Frequency (n) | Percentage (%) |
| Information received before first menstruation | Yes | 504 | 81.0 |
| No | 121 | 19.0 | |
| Age at menarche | Before 11 years | 52 | 8.0 |
| 12–14 years | 457 | 73.0 | |
| 15–16 years | 111 | 18.0 | |
| Above 16 years | 5 | 1.0 | |
| Normal bleeding during last menstrual cycle | Yes | 518 | 83.0 |
| No | 107 | 17.0 | |
| Menstrual complications | Menorrhagia | 144 | 23.0 |
| Oligomenorrhea | 172 | 28.0 | |
| Polymenorrhea | 136 | 21.0 | |
| Multiple complications | 173 | 28.0 | |
| Family history of dysmenorrhea | Yes | 353 | 56.0 |
| No | 272 | 44.0 | |
| Menstrual bleeding duration | <3 days | 65 | 11.0 |
| 3–5 days | 426 | 68.0 | |
| >5 days | 134 | 21.0 | |
| Severe pain during menstruation | Yes | 420 | 67.0 |
| No | 205 | 33.0 | |
| Medication during menstruation | Yes | 261 | 42.0 |
| No | 364 | 58.0 | |
| Food consumption during menstruation | Less | 289 | 46.0 |
| Unchanged | 225 | 36.0 | |
| More | 111 | 18.0 | |
| Menstrual management material | Disposable | 458 | 73.0 |
| Reusable | 167 | 27.0 |
Figure 2 illustrates the distribution of the menstrual needs score between the users of disposable and reusable materials in the study. Both the visual inspection and the independent T-test (p > 0.05) confirmed there is no significant mean difference in the overall needs score based on the type of materials used. However, subsequent multivariable linear regression analyses identified significant differences in specific MPNS-36 domains and the adjusted overall score after controlling for socio-demographic and menstrual characteristics, suggesting that these factors may influence the relationship between menstrual material type and menstrual needs.
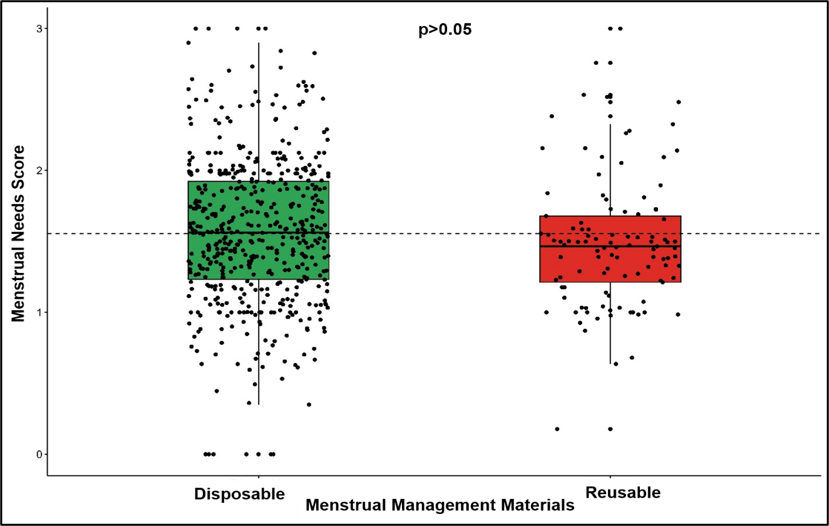
Figure 2. Distribution of menstrual needs score between disposable and reusable materials users.
Table 3 shows that, after adjustment for socio-demographic and menstrual factors, the use of reusable menstrual materials was associated with significantly lower scores, indicating worse menstrual needs experiences across several key domains compared with disposable material use. Specifically, reusable material users had lower scores for material and home environment needs (β = −0.21, 95% CI: −0.34, −0.09; p = 0.001), transport and university environment needs (β = −0.18, 95% CI: −0.30 to −0.05; p = 0.006), and reuse needs (β = −0.23, 95% CI: −0.39, −0.06; p = 0.007). The overall menstrual needs score was also significantly lower among reusable material users (β = −0.12, 95% CI: −0.20, −0.03; p = 0.010), suggesting a consistently poorer needs experience in this group. In contrast, no significant differences were observed for material reliability concerns (β = −0.04; p = 0.511), change and disposal insecurity (β = 0.02; p = 0.741), or reuse insecurity (β = 0.13; p > 0.90), indicating that these aspects of menstrual needs did not vary by type of menstrual material used.
Table 3. Association between menstrual needs and menstrual materials used by the participants (N = 625).
| Menstrual Needs | β1 | 95% CI2 | P-value* |
| Material & Home Environment Needs | -0.21 | -0.34, -0.09 | 0.001 |
| Transport & University Environment Needs | -0.18 | -0.3, -0.05 | 0.006 |
| Material Reliability Concerns | -0.04 | -0.18, 0.09 | 0.511 |
| Change & Disposal Insecurity | 0.02 | -0.10, 0.14 | 0.741 |
| Reuse Needs | -0.23 | -0.39, -0.06 | 0.007 |
| Reuse Insecurity | 0.13 | -0.16, 0.16 | > 0.9 |
| Overall | -0.12 | -0.20, -0.03 | 0.010 |
| 1Adjusted for socio-demographic and menstrual variables; The reference category is disposable. CI = Confidence Interval; *Significant values (p < 0.05) are in bold. | |||
The findings from this study highlight significant differences in menstrual needs and insecurities between users of disposable and reusable menstrual materials. After adjusting for socio-demographic and menstrual factors, users of reusable materials reported consistently poorer experiences across several key domains compared to disposable material users. Specifically, reusable material users had significantly lower scores related to material and home environment needs, transport and university environment needs, and reuse needs. Similar findings were found in global university settings and across diverse international contexts [18-20]. These results suggest that reusable menstrual materials may pose greater challenges in managing menstrual hygiene effectively within personal and external environments. To facilitate interpretation of the study findings and their public health implications, Figure 3 presents a conceptual framework synthesized from the observed associations between menstrual product type and menstrual hygiene management needs among female university students in Bangladesh.
The lower scores for material and home environment needs among reusable material users indicate potential difficulties in accessing or maintaining suitable facilities and resources at home, including a lack of water, sanitation, privacy, cleaning supplies, and discreet laundering spaces, which hinder maintenance and use. These issues were also reported in India [21] and Nigeria [22]. The decreased scores in transport and university environment point to barriers in managing menstruation comfortably and securely in public or institutional settings, which could impact academic participation and daily functioning that has been reported by women across global settings [23], even in developed countries like the United States of America [24] and the United Arab Emirates [25]. The significantly poorer reuse needs experienced by reusable material users further emphasize the complexities involved in cleaning, drying, and storing reusable materials, which may contribute to discomfort or health concerns. This issue has been significantly noticed in LMICs like India, South Africa, Tanzania, Kenya, and Uganda [26].
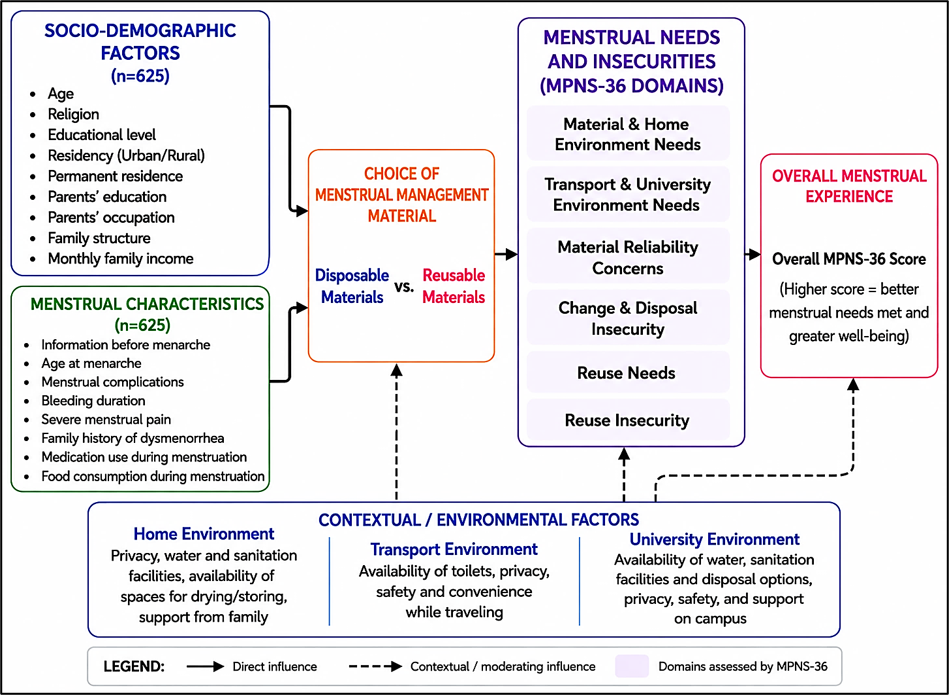
Figure 3. Conceptual framework illustrating the relationship between menstrual product type and menstrual hygiene management needs among female university students in Bangladesh.
Interestingly, no significant differences were found between the two groups in terms of material reliability concerns, change and disposal insecurity, or reuse insecurity. This suggests that while reusable materials are associated with challenges in specific practical and environmental aspects, perceptions of reliability and security in changing or disposing of menstrual materials do not differ markedly from those of disposable material users. Researchers in Australia found similar results [27] and Spain [28]. This may reflect acceptance or normalization of certain insecurities regardless of menstrual product type or could indicate that factors beyond the type of menstrual material influence these insecurities. The high prevalence of severe menstrual pain, family history of dysmenorrhea, and medication use reported among participants underscores the broader context of menstrual health challenges faced by the study population. These factors may exacerbate the difficulties experienced by reusable material users, potentially compounding menstrual management needs and insecurities [29-31]. However, these findings should be interpreted within the Bangladeshi context, where menstrual experiences are strongly shaped by cultural norms, stigma, and access to supportive facilities. Therefore, local contextual factors may play a more influential role in shaping menstrual insecurities than the specific menstrual material used.
Several limitations should be considered when interpreting the findings of this study. First, the cross-sectional design precludes causal inference between menstrual material type and menstrual needs experiences. Second, data were self-reported and therefore subject to recall and social desirability biases, particularly given the sensitive nature of menstruation. Third, although participants were recruited from universities across multiple administrative divisions of Bangladesh, the study population consisted exclusively of university students, which may limit the generalizability of the findings to adolescents not enrolled in higher education, women from lower educational backgrounds, or older reproductive-age populations. Fourth, clustering at the university level was not explicitly modeled during the analysis because the study primarily focused on pooled individual-level estimates; therefore, some residual clustering effects cannot be entirely excluded. Finally, important contextual factors such as the quality of water, sanitation, and hygiene facilities, cultural beliefs surrounding menstruation, and product affordability were not directly measured and may have influenced participants’ experiences. Despite these limitations, the study provides baseline evidence on menstrual needs and insecurities among female university students in Bangladesh using a validated menstrual health assessment tool.
This study demonstrates that female university students using reusable menstrual materials in Bangladesh face significantly greater challenges in meeting their menstrual needs compared with disposable material users, particularly in the home, transport, and university environments. While reusable products are often promoted for their affordability and environmental benefits, the findings suggest that inadequate infrastructure, limited privacy, and difficulties related to cleaning and reuse may undermine their effective and dignified use. The absence of differences in certain insecurity domains indicates that some menstrual concerns persist regardless of product type. Overall, these results underscore the importance of coupling menstrual product promotion with investments in water, sanitation, hygiene facilities, and menstrual health education to ensure equitable and safe menstrual hygiene management for young women.
The authors sincerely thank all female university students who voluntarily participated in this study and generously shared their experiences. We also acknowledge the support of the respective universities and individuals who facilitated participant recruitment and data collection. The authors are grateful to all research assistants and collaborators whose contributions supported the successful completion of this study.
This study received no external funding at any stage of the publication process.
The authors report no commercial or non-financial conflicts of interest.
This study received ethical approval from the Biosafety, Biosecurity, and Ethical Committee of Jahangirnagar University (Ref No: BBEC, JU/M 2023/ 12 (77)) before the data collection. Informed consent and voluntary participation were ensured. All participants in this study provided written informed consent for the publication of their data in anonymized form. They were assured that no identifying personal information would be published. Participants were informed of their right to withdraw consent at any time, without affecting their involvement in the study.
Md. Mahadi Hassan (MMH): Conceptualization, Methodology, Formal Analysis, Data Curation, Visualization, Writing – Original Draft, Writing – Review & Editing. Noushin Nohor (NN): Writing – Original Draft, Writing – Review & Editing. Raiyaan Tabassum Imita (RTI): Writing – Original Draft, Writing – Review & Editing. Md. Fakhrul Islam Maruf (MFIM): Writing – Original Draft, Writing – Review & Editing. Anika Bushra Boitchi (ABB): Supervision, Writing – Review & Editing. All authors have read and approved the final version of the manuscript.
The authors used open AI solely for language editing, grammar correction, and improving readability. All AI-assisted content was carefully reviewed and validated by the authors, who take full responsibility for the manuscript. No AI tool was used for study design, data collection, data analysis, interpretation of results, or generation of scientific conclusions.
The dataset and materials used and analyzed during the study are available from the corresponding author upon reasonable request. The lead author, Md. Mahadi Hassan affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted.

This work is licensed under a
Creative Commons Attribution 4.0 International License
.
You are free to share and adapt this material for any purpose, even commercially, as long as you give appropriate credit.
 access
access